

Introduction
Red cell rheology is abnormal in sickle cell disease (SCD); red blood cells (RBC) are rigid, dense, and the sickle hemoglobin (HbS) polymerizes with deoxygenation. There are several devices commercially available and under development to assess RBC rheology. One is an oxygen gradient ektacytometer (Lorrca with Oxygenscan, RR Mechatronics) which measures RBC deformability under oxygenated conditions (EImax) and deoxygenated conditions (EImin), and the oxygen concentration at which deformability begins to worsen, point of sickling (PoS). A commercially available hematology analyzer, the ADVIA (Siemens), measures hemoglobin (Hb) by flow and colorimetric methods, permitting automated calculation of the percent dense red blood cells (%DRBC). Allogeneic hematopoietic stem cell transplant (alloHSCT) can provide a cure for SCD, and viable gene-based therapy options are under investigation to serve the many patients without a matched related donor. However, the level of HbS correction or functional Hb induction necessary to achieve a cure is still unknown. Clinical endpoints such as prevention of pain events are important, but it is possible to be pain free for several years while still experiencing organ damage. As gene-based therapy clinical trials move forward, we must assess the level of functional improvement beyond Hb profile and conventional clinical labs. We propose that the goal of any gene-based SCD therapy should be to normalize blood rheology to the level of an individual with sickle cell trait (HbAS), and that EImax, EImin, PoS, and %DRBC may be used to distinguish between HbAS and HbSS/Sβ0 genotypes.
Methods
Subjects: Blood samples were collected from 257 unique patients (17 HbAS, and 240 HbSS/Sβ0) under IRB-approved protocols at Texas Children's Hospital and University Medical Center Utrecht. Patients were 56% male, ages 9 months to 22 years. Some HbSS/Sβ0 subjects were on transfusion and hydroxyurea (HU) (Table 1). Fetal hemoglobin (HbF) levels ranged from 0-41%.
Oxygen gradient ektacytometry: Blood collected in EDTA and standardized to a fixed RBC count was suspended in 5 mL polyvinylpyrrolidone at room temperature. 1.5 mL of the sample solution was injected into test cup. Each sample was run in duplicate.
ADVIA: 250µL of blood collected in EDTA at room temperature was aspirated to measure the %DRBC, defined as the percentage of RBCs with a Hb concentration >1.11 mg/mL.
Analysis: Patient characteristics were summarized using median with 25th and 75th percentiles, and frequency with percentage. Characteristics and labs were compared by group with t-test, Wilcoxon rank sum test, or Fisher's exact test. Receiver operating characteristics (ROC) analyses were performed to identify HbAS versus HbSS/Sβ0 for each biomarker. All analyses were performed using Stata 15.
Results
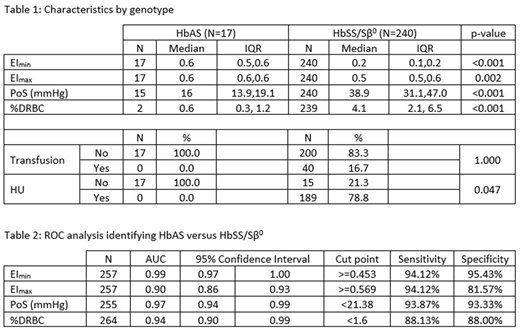
The EImin, EImax, PoS, and %DRBC differed significantly between the HbAS and HbSS/Sβ0 groups, despite including transfused, very young, and HU-treated samples in the HbSS/Sβ0 cohort (p<0.001, p=0.002, p<0.001, and p<0.001, respectively; Table 1).
ROC analysis showed that a threshold Elmin greater than or equal to 0.453 identified HbAS with 94.12% sensitivity and 95.43% specificity. EImax greater or equal to 0.569 identified HbAS with 94.12% sensitivity and 81.57% specificity. PoS less than 21.38 mmHg identified HbAS with 93.87% sensitivity and 93.33% specificity. %DRBC less than 1.6% identified HbAS with 88.13% sensitivity and 88.00% specificity (Table 2).
Conclusion
Conventional laboratory testing may not be able to establish if gene-based therapy has achieved a cure. We propose to define a cure as achievement of an HbAS level of RBC quality in a gene-based therapy edited RBC population. We show that rheological biomarkers EImin, EImax, PoS, and %DRBC differ significantly between individuals with HbAS and HbSS/Sβ0 of all spectrums of severity and treatment regimens. Not only are the rheological biomarker values significantly different, but there is little to no overlap in ranges of values obtained from the different genotypes, even in heavily transfused HbSS patients, with HbS as low as 31%. EImin, EImax, PoS, and %DRBC functionally identify genotype with high sensitivity and specificity; we propose that they be used not to diagnose SCD, but to determine if a HbSS or HbSS/Sβ0 individual who has undergone successful gene-based therapy has achieved the RBC functionality of a HbAS individual.
van Beers:Novartis: Research Funding; Pfizer: Research Funding; Agios: Membership on an entity's Board of Directors or advisory committees, Research Funding; RR mechatronics: Research Funding. Wijk:Agios Pharmaceuticals Inc.: Research Funding; RR mechatronics: Research Funding. Rab:RR Mechatronics: Research Funding. Sheehan:Global Blood Therapeutics: Research Funding; Novartis: Research Funding; Emmaus: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal